Two decades ago, a small group of Tamil professionals in the United States asked a simple question: instead of meeting and eating, why not do something for our people? What grew from that conversation has transformed hospitals, restored sight, saved hearts, and quietly rewritten the story of a community that war nearly erased.
By: Aruliniyan Mahalingam
I have no formal connection to the medical profession. Yet, in a way that feels almost inevitable, I have always found myself surrounded by doctors—within my family, among my friends, and across the circles I move in.
Over time, as I began engaging with them more closely—first out of curiosity, then as a journalist, and eventually as a friend and well-wisher—I was drawn into the world of healthcare stories in Sri Lanka, particularly in the North and East.
Almost every time I covered an issue related to health or well-being in Jaffna or elsewhere in the North and East, one name kept resurfacing: IMHO — the International Medical Health Organization.

At first glance, the scale of its work was misleading. The reach, the consistency, the depth—it all suggested something far bigger. I assumed IMHO was a global institution, well-funded by states and international actors, something akin to Médecins Sans Frontières, backed by vast networks and deep resources.
But the truth was far more compelling.
IMHO was not a distant international giant. It was, in fact, the creation of a small group of Sri Lankan Tamil professionals abroad—individuals who had chosen, in their own way, to respond to a broken system.
In many ways, IMHO is doing the kind of work one would expect from a state—or from a powerful international agency. Only here, it is being carried out quietly, consistently, and almost entirely through collective will.
THE ROAD BACK TO JAFFNA

In 2002, following a ceasefire between the Liberation Tigers of Tamil Eelam and the Sri Lankan government, some who had left the country were able to return home for the first time in years. Dr. Rajam Theventhiran—a psychiatrist based in New York City and one of the founding board members of IMHO—was among them.
What she found was shocking—even to those who had followed the reports from afar. The Jaffna district, home to roughly 600,000 people and once one of the most educationally advanced regions in South Asia, had been comprehensively broken.
Jaffna Teaching Hospital—the only tertiary care centre for the entire Northern Province, serving five districts across hundreds of kilometres—had been displaced twice during three decades of conflict. Its buildings had come under artillery fire; at one point, it had witnessed a brutal massacre during the Indian Peace Keeping Force (IPKF) period.
A report from the mid-2000s, Dr. Rajam told me, estimated that 38 peripheral hospitals across the district were being managed collectively by just 14 doctors. Medications were scarce. Equipment was lacking. In rural areas, even travel was a gamble—landmines still lay buried beneath the soil.
“When we had left the country, it had been in a much better condition. We felt a strong sense of responsibility. Perhaps that responsibility took shape in IMHO,” Dr. Rajam told me. “Rajam Akka has given her life to IMHO,” a doctor friend told me. “She breathes it, thinks about it all the time, goes to bed, and wakes up with new ideas related to its work.
A MOTHER IN MULLAITIVU
The room from which Dr. Rajam tells me these stories—through a flickering Zoom window—is worlds away from the landscapes, memories, and the immense work she carries within her.
She speaks from the United States, from the quiet order of a diaspora life. But her words travel elsewhere. They return to Mullaitivu—to the flat, salt-tinged coastline of Sri Lanka’s north, a region that witnessed not only the brutal final chapter of the Sri Lankan war but also nature’s fury, when the 2004 Indian Ocean tsunami swallowed homes, erased shorelines, and upended entire lives.
“There was a mother,” she began, her voice slowing under the weight of what she was about to say. A pause. “There was a mother… She had lost all six of her children to the tsunami.”
Dr. Rajam had returned then as part of the relief effort—not only to deliver aid, but also to sit with people and listen. She sat with that mother in the aftermath of unimaginable loss. What the woman said next has never left her.
“She told me,” Dr. Rajam recalled, “that although she had lost all six of her children, she had found some peace… because she believed that God takes good people at a young age.”
“That was her way—her faith, her philosophical explanation for something so unimaginable,” Dr. Rajam told me. “I think of her often. Even today—when you texted me about this interview—that mother came to my mind. She gave me a lesson I have carried all my life.”
A silence settled between us.
“Even in the deepest cruelty, there is still hope.” Dr. Rajam told me.
It lingered in the air. Perhaps that is where IMHO’s charter lies—in that quiet, stubborn insistence on hope. A refusal to look away from suffering. A willingness to sit with it. And, above all, the resolve not just to witness, but to act.
Then, with a calm certainty that carried years behind it, she said, “IMHO is in the business of giving hope. And we have been in this business for quite a long time.”
THE FOUNDING

In September 2003, Rajam Theventhiran sat down with Dr. Thavam Thampi Pillai—a transplant surgeon and current President of the International College of Surgeons—along with Dr. S. Raguraj, an internist, and Dr. Sujanthy Rajaram, a specialist in both internal medicine and critical care. None of them had experience running a charity. What they had instead was a shared unease—a sense that something had to be done.
They debated names, turning over possibilities, before settling on the International Medical Health Organization—IMHO. From the outset, they were clear: this would not be an organisation confined by race, ethnicity, or even national boundaries. The work, they believed, had to travel wherever it was needed. And the name aptly reflected that.
“I returned to Sri Lanka in 2003, after sixteen years,” Dr. Thavam Thampi Pillai told me. “During that visit, I went to Jaffna Teaching Hospital. On rounds with Dr. Perandarajah, I saw a young boy—perhaps in his early teens—diagnosed with kidney failure.”
“At the time, there was no dialysis or transplant available in the public sector in Sri Lanka. It was hard for me to come to terms with the fact that a young boy was going to die of a benign illness, which, in another setting, would be a manageable condition. He had a worse prognosis than many of the cancer patients we treat in the West. That harsh truth shattered me completely.”
He pauses.
“It became one of the key reasons I went on to help co-found IMHO.”
“Jaffna Teaching Hospital was, in many ways, ahead of its time,” Dr. Thavam Thambi Pillai told me. “As far back as 1977, it had been performing advanced thoracic surgeries under Dr. Narkunam. Had that trajectory continued, by 2003 the hospital might have been performing heart transplants.”
But the reality was starkly different. Years of conflict had pushed it back by decades. Instead of performing advanced surgeries, doctors were watching children die from treatable conditions.
“There was a deep sense of sadness—that we had gone back in time,” Dr. Thavam Thambi Pillai said. “A sense of betrayal, on my part, for having left the land. And perhaps even guilt.”
“It was that emotional reckoning that became a turning point in my life,” he continued. “I could see the immense level of need. And I knew I could not address it alone. So, I sat down with my friends and well-wishers—and we began IMHO.”
Not a Doctors’ Organisation
At first glance, IMHO sounds like what many assume it to be—an organisation of doctors, by doctors, for doctors. But that assumption does not hold.
“We are not just a doctors’ organisation,” Dr. Thavam Thampi Pillai told me. “Many of us come from medical backgrounds. But IMHO was never meant to be limited to that.”
There is no formal membership structure. No rigid professional boundaries. No gatekeeping. The organisation is governed by a ten-member board—bringing together not just doctors, but also accountants, engineers, university lecturers, and others from diverse walks of life, Dr.Rajam told me.
“None of us from IMHO-USA receive any compensation,” Dr. Rajam said, “We are one hundred percent volunteers—and we will remain so for life.”
THE FIRST PROJECT—AND WHAT IT BECAME

Their first project reflected a clear philosophy.
“The backbone of any healthcare system—whether in a high-income country or a low-income one—is primary care,” Dr. Thavam Thambi Pillai told me.
So, they decided to build a primary healthcare centre—and run it free of charge.
During the ceasefire period, when travel to the North became possible, they identified a war-affected area in Mullaitivu—Iyankankulam—as the site. The cost was estimated at around $75,000 to build, with an additional $1,500 a month to maintain it.
Free medication, he explained, was essential. “If someone is struggling to put food on the table and you ask them to buy blood pressure medication, they simply won’t take it—unless you provide it.”
Then came the harder question: how to raise the money.
IMHO organised its first fundraising dinner. A plate cost $1,000. Thirteen people attended. They raised $13,000.
It was a start—but far from enough.
So, they organised a second fundraiser. This time, they did something different. “We didn’t fix an amount,” Dr. Thavam Thampi Pillai told me. “People told us—we are asking for too little. Just open it up. Let people give what they want.”
Within a few fundraisers, the full $75,000 had been raised!

Then came an unexpected phone call. A man offered to sponsor an entire primary healthcare centre—$75,000. It was Mr. J. M. Rajaratnam, father of Raj Rajaratnam, the former Wall Street financier.
A month later, at a fundraiser in upstate New York, another $75,000 was raised.
“That’s when we realised—maybe we are onto something,” he said. “I was reminded of a line from The Alchemist by Paulo Coelho: ‘And, when you want something, all the universe conspires in helping you to achieve it.’ It felt like that—the universe helping us, through a few good Samaritans.”
What began with thirteen plates and thirteen thousand dollars has since grown—by Dr. Rajam own accounting—into more than fifteen million US dollars in total interventions, across Sri Lanka and nineteen other countries, funded almost entirely by individual Tamil donors.
THE TSUNAMI YEAR
Fourteen months after IMHO was founded, the Indian Ocean tsunami struck on the morning of December 26, 2004. The Sri Lankan coast was among the worst affected in the world. The north and east bore a particularly heavy toll.
Within two weeks, Dr. Rajam and others were on the ground.
Some went to Kilinochchi. Others moved across the north and east. They bought vehicles and medicines. They set up camps. They drove through a coastline that looked, in places, like a war zone.
“It was a huge crisis,” Dr. Rajam told me. “But within a very short time, we were able to collect enough funds, buy vehicles and medicines, and travel to Sri Lanka. Within two weeks, we were there.”
The tsunami expanded IMHO’s sense of its own purpose. It also sharpened its instincts.
“This showed us the importance of an organisation like IMHO,” she said. “It showed us that we could make a difference—that we could do something meaningful to help people.”
But it also taught them something else.
That they could move fast—faster than larger institutions, often slowed by bureaucracy.
When the ceasefire eventually collapsed, and the A9 highway connecting Jaffna to the south was closed by the military, IMHO managed to send the first emergency shipment of psychiatric medication into the North.
When hundreds of thousands were crowded into the Manik Farm, an internally displaced persons camp in Vavuniya after the war’s bloody end in May 2009, IMHO was working on water, sanitation, and nutrition within days, well before any international NGO could start operations.
“Do you know who suffers the most during wartime?” Dr.Rajam asked. “It is those requiring long-term care—patients with mental illness, cancer, and renal disease, as well as the elderly, children, and pregnant.”

During the final and most devastating phase of the war, reports began to emerge from the War Zone—stories of acute suffering, particularly among women and children. IMHO managed to send a shipload of milk powder into the war zone, which reached civilians on April 1, 2009. A second consignment was dispatched—but it never reached its destination. By mid-May, the war had come to an end.

DIGNITY IN THE CAMPS
When the war ended, the crisis did not.
Hundreds of thousands of displaced people were moved into camps. The largest of them was Manik Farm. In Jaffna, too, camps filled with people who had lost everything—including, for many women, even the most basic conditions for safe childbirth.
One project from those difficult months of 2009 has remained especially close to Dr. Rajam’s heart.
When displaced families were brought to Jaffna and placed in camps, there were hundreds of pregnant women among them. The Regional Director of Health Services, Dr. Keetheswaran, wanted to convert a small divisional hospital in Varani into a maternity centre—to spare these women from giving birth in tents, under the harsh summer heat.
He reached out to IMHO.
There was no bureaucracy to slow things down.
Within hours, the board had approved the funding. The money was transferred. The hospital was converted.
Nearly a hundred mothers delivered their babies there. They were given home-cooked meals—and, for the first time in months, the dignity of a proper recovery.
Dr. Rajam told me this project remains deeply personal to her.
“As a woman, I have always felt that in vulnerable moments, it is not only survival that matters—dignity matters too.”
For her, the significance of the project goes beyond numbers.
“It also taught us something important,” she added. “Even a small amount of money—if used at the right time, for the right need—can have a very large impact.”
It is a lesson, she said, that has guided IMHO’s work for more than two decades.
THE HEART OF JAFFNA
Among the most remarkable contributions IMHO has made in the North is the establishment of a functional cardiac catheterisation laboratory.
In 2008, cardiologist Dr. Lakshman approached the organisation. The A9 highway was still closed. The nearest cardiac catheterisation facility was in Colombo—over four hundred kilometres to the south. For a Tamil patient in Jaffna suffering a heart attack, the choices were stark: make the costly and uncertain journey south, or risk death. Many faced the latter.
The catheterisation laboratory required over $600,000. The board began raising funds, reaching out to donors in Boston, New York, Toronto, and London—Tamil families who understood what it meant to live without access to advanced care. They raised enough to construct the building. The Canadian International Development Agency supported the construction. Later, when the French government decided to donate two cath labs to Sri Lanka, Jaffna received one—largely, insiders believe, because the infrastructure was already in place.
The unit opened around 2011. Today, the cardiology centre at Jaffna Teaching Hospital is among the most functional in the country. It draws patients not only from the Northern and Eastern provinces, but also from the North Western and Southern regions. There are no long waiting lists for catheterisation. Bypass surgeries—once unthinkable in Jaffna—are now performed there.
Paediatric cardiologists and cardiac surgeons have since joined the staff—drawn partly by the facility’s reputation, and partly by the knowledge that something real and lasting had finally been built in a place long denied both.
“Start small, but with sincerity,” Dr. Thavam Thambi Pillai said. “That has always been one of our guiding principles—and it will grow.”
The same principle led to the establishment of the diabetes centre at Jaffna Teaching Hospital. In 2008, Dr. Sivansuthan, a consultant physician, approached IMHO with a troubling observation: more than fifty percent of diabetes patients were seeking treatment only at very late stages—often when amputation had already become necessary.
IMHO, arranged for him to visit a diabetic centre in Dayton, Ohio. Upon his return, the organisation funded renovations and staff salaries to help establish a dedicated diabetic centre.
In 2015, a fully qualified endocrinologist, Dr. Mahalingam. Aravinthan joined the unit. This year, another specialist has followed. The centre now functions with a level of institutional momentum that was once unimaginable.
THE WORLD HEALTH ORGANIZATION TOOK NOTICE
IMHO’s work in mental health has been, in many ways, the least visible aspect of what it does.
In post-conflict societies, mental illness remains a vast and chronically underfunded public health challenge. In Tamil society, as in many others, stigma only deepens the suffering.
“We do many projects related to mental health,” Dr. Rajam Amma told me with a faint smile. “Sometimes our friends joke—half seriously—that IMHO stands for the International Mental Health Organization.”
Soon after the tsunami, when IMHO contacted Dr. Ganesan, a psychiatrist in Batticaloa, he requested support to complete an inpatient psychiatric unit that had originally been initiated by the World Health Organization.
Since then, IMHO has supported mental health programs in Batticaloa, Vavuniya, Negombo, Angoda and Maskeliya under his guidance.
In Vavuniya, IMHO funded the first inpatient psychiatric unit in a stretch of more than a hundred and fifty kilometres that had no such facility—a region where most patients spoke Tamil and the nearest care was delivered in Sinhala. The unit cost fifty thousand dollars and was opened just before the end of the 2009 war. During the months that followed, when hundreds of thousands of displaced people were processed through Manik Farm, that unit served patients who had nowhere else to go.

In the years following the war's end, IMHO worked extensively with Dr. Sivayogan, a psychiatrist in Jaffna. One key initiative was Kudil—a rehabilitation service for people with severe mental illness, operating on the understanding that clinical treatment without social rehabilitation leaves most patients stranded in a recovery that has nowhere to go. The Kudil project in Tellipalai cost $450,000. It was funded entirely by a single family, in memory of their parents. It opened in 2022.
"When you visit," Dr. Rajam says quietly, "what stands out is not just the care, but the dignity and hope these individuals regain.
The World Health Organization has cited Kudil in a blog post as a model for mental health rehabilitation in Southeast Asia. More recently, Dr. Sivayogan highlighted the need for a dedicated facility for patients without family or community support. IMHO supported the construction of a new centre, “Thoomani Maadam” at $110,000, funded by a single donor. It opened last year and is already fully occupied.
Expanding the Meaning of Care
IMHO did not confine itself to medicine alone. Over time, it came to recognise that health cannot be treated in isolation—that medical outcomes are deeply tied to education, water, sanitation, and the broader conditions in which people live. Without addressing these, meaningful healthcare remains out of reach.
“If you ask me to classify our main areas of work,” Dr. Rajam told me, “I would say they fall into three broad categories: health, education, and community development—with water, sanitation, and livelihoods forming a key part of that third category.”
“In the beginning, we focused mainly on medical needs. But over time, we evolved naturally. We realised that health, in its true sense, is not possible without clean water, proper sanitation, education, and economic empowerment.”
That shift began to take shape around 2010, as communities slowly resettled after the war.
One of IMHO’s early interventions was in Sampur, in the Trincomalee district. There, the organisation built 139 shelters and about 50 toilets. Since most residents were fishermen, IMHO also provided fishing boats and nets—supporting around 50 families to rebuild their livelihoods.
Similar work followed in Batticaloa. In Parankiyamadu, in 2020, many resettled families lacked even basic sanitation. IMHO helped build 47 toilets and around 30 shelters, while also supporting livelihoods—again, primarily through fishing boats.
In total, more than 200 families have received fishing boats—targeted at resettled and vulnerable communities.
Support for persons with disabilities became another critical area.
In the immediate post-war years, IMHO worked with Mannar and Vavuniya hospitals, as well as the Jaipur Centre, to address urgent rehabilitation needs. They provided equipment, supported physiotherapists’ salaries, and collaborated with multiple organisations.
One such collaboration was with the Mehta Foundation, led by Dr. B. Panagamuwa, a Sinhalese doctor, who continues his work today, running a limb-fitting centre in Kilinochchi.
IMHO also partnered with a UK-based organisation, Motivation charitable Trust, to provide wheelchairs.
Among those most affected were men and women left paraplegic or quadriplegic by war injuries. Many of them came together to form their own organisation—a quiet act of resilience in itself.
Since 2012, IMHO has worked closely with this group, helping restore a sense of independence long out of reach. Thirty three-wheelers (auto rickshaws) were provided to improve mobility for paraplegic patients—enabling them not only to move, but to earn a livelihood. For many, it marked the first real opportunity to stand on their own, both economically and emotionally.
“One recipient once told us,” Dr. Rajam recalled, “not only has IMHO given us dignity, but you’ve given us our legs back.”
In addition, around 30 specially designed bathrooms were constructed, and access to clean water was secured—small interventions, but transformative in their impact.
It is difficult to hear such words and remain unmoved—especially when they come from those who have endured the long shadow of three decades of war, Dr. Rajam told me.
At their centre in Mangulam, a small medical unit treats bedsores—common among those who are wheelchair-bound or bedridden. Since around 2019, IMHO has supported staff salaries and, during times of economic hardship, even medication.
These were not large, visible projects—but they addressed deeply human needs.
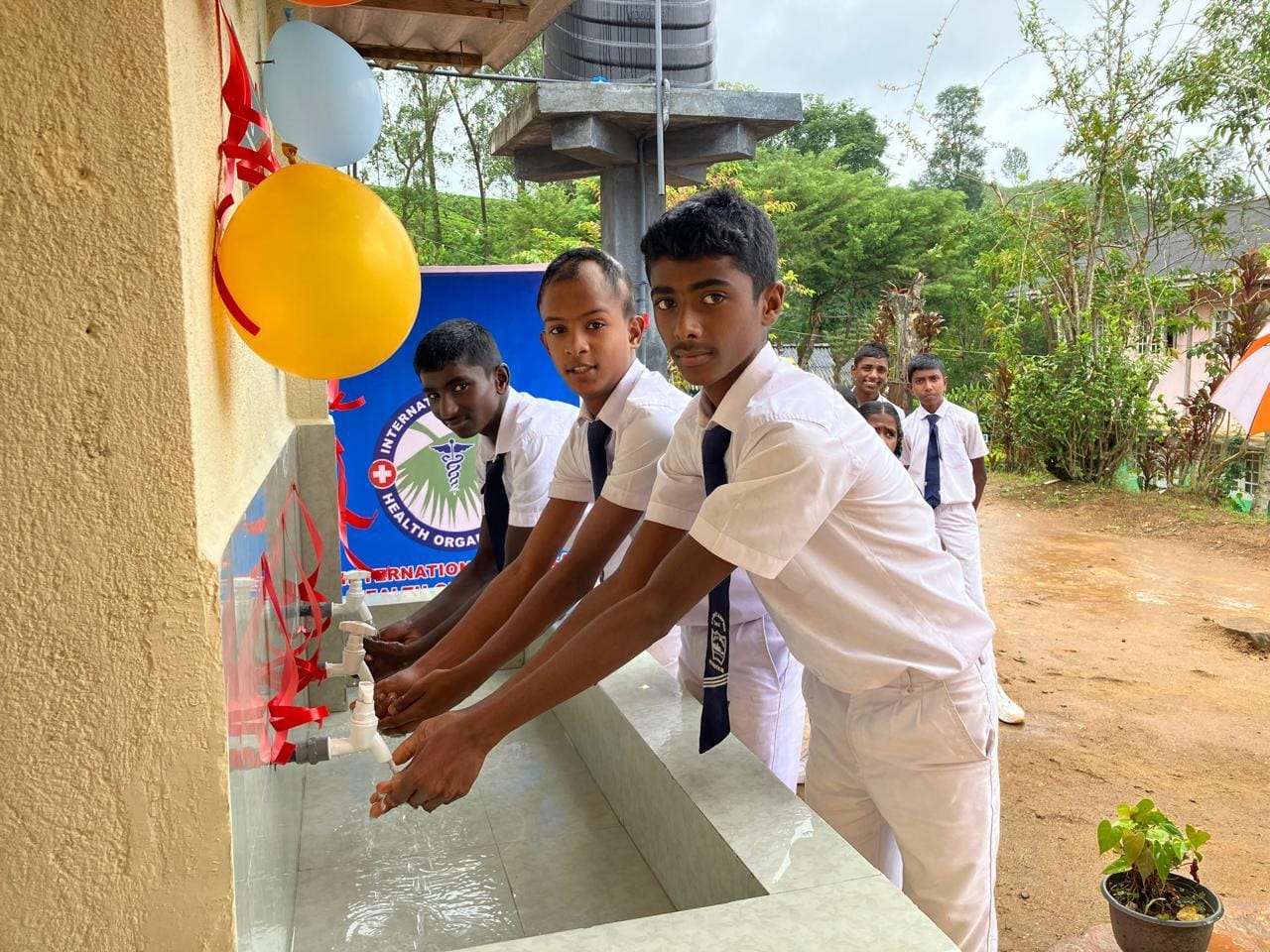
At the same time, IMHO expanded its work in water and sanitation across the North, East, and upcountry regions.
But increasingly, another priority began to take shape: education.
“Our education work falls into two broad areas,” Dr. Rajam said. “Early childhood education and school-level support.”
So far, IMHO has supported at least 65 preschools—helping with infrastructure, learning materials, and teacher training.
It has also expanded into STEM education. In partnership with the UK-based Ratnam Foundation, IMHO has provided smart boards to nearly 300 schools.
Capacity-building is another focus. Training programmes range from preschool teachers to English teachers—aimed at improving the quality of education across all levels.
But the deeper issue, she said, is access.
“We often say education is the most powerful tool to fight poverty. But many children still don’t have access to it,” Dr. Thavam Thambi Pillai told me.
It is a line that echoes a familiar truth. Nelson Mandela once said, “Education is the most powerful weapon which you can use to change the world.” Yet, for many children, that weapon remains out of reach.
In some of the most vulnerable areas, dropout rates climb to nearly 40 percent.
The reasons are rarely simple. Hunger. Long and costly journeys to school. Crumbling infrastructure. Classrooms without furniture. Schools without proper water or sanitation.
“So, we try to address all of it,” Dr. Rajam said.
In the upcountry, IMHO supports around 75 high school students with scholarships—helping cover transport and tuition. In Vavuniya, where children often travel long distances in search of better schools, the organisation funds a school bus for nearly 90 students, covering fuel and the driver’s salary.
“These may seem like small interventions,” she said. “But they fill critical gaps—and make a real difference.”
THE UPCOUNTRY AND THE MATHEMATICS OF DIGNITY

In 2016, IMHO expanded its work into Sri Lanka’s upcountry tea-growing regions—home to Tamil communities brought by British colonial planters from South India in the nineteenth century.
What it encountered there did not fit neatly into the organisation’s existing framework, which had been shaped largely by post-conflict needs in the North and East. The problems in the hill country were different in character: deep, generational poverty; a persistent water crisis in schools; and dropout rates approaching forty percent—driven by a web of interconnected causes that could not be addressed in isolation.
“We are, in many ways, indebted to Sri Lanka’s free education system—something most of us in IMHO have benefited from,” Dr. Rajam told me. “But we must also acknowledge that this system has been sustained, in part, by the foreign exchange brought in by the tea industry.”
“The cruel irony is that the very people who generate that wealth continue to live in conditions of deep poverty.”
These upcountry Tamil communities remain among the most marginalised in the country—living in conditions that successive governments have, for decades, failed to meaningfully address.
For IMHO, the decision to enter the hill country was shaped not only by need, but by a sense of obligation.
“We cannot solve every problem,” an IMHO official told me. “But we felt we had to try—at least in some small way.”
The reasons, she explained, are deeply interconnected: lack of food, transport difficulties, poor infrastructure, absence of basic furniture, lack of teaching staff, and inadequate water and sanitation.
IMHO responded by addressing these gaps simultaneously.
It built water supply systems in thirty-five schools. It constructed nearly 1,500 toilets—around 700 in collaboration with Rotary International. It began supporting 380 children between the ages of three and eighteen—all of them orphans or children of single parents—with a monthly allowance of 3,000 rupees, largely in the form of dry rations, tied to one condition: stay in school.
Then something unexpected happened.
The women in these communities did not ask for more aid. They asked for a way to save.
IMHO helped establish savings groups, forming ninety groups that brought together over 1,000 members. In 2019, they opened a cooperative store, which continues to operate. In 2022, a vocational training centre was established in Maskeliya. By last year, the initiative had expanded into small-scale manufacturing—producing garments, bags, shoes, and, more recently, sanitary pads, using machinery imported from India.
The sanitary pad initiative emerged from a recurring concern.
“Many schoolgirls were missing classes during their menstrual periods,” Dr. Rajam told me, “because they could not afford sanitary products—and because school toilets were either absent or lacked basic privacy.”
So far, IMHO has provided sanitary pads to nearly 1,000 girls and women.
“We do not see this merely as a distribution project,” she said. “We see it as an initiative for women’s dignity and empowerment.”
Among those who benefited from IMHO’s support is a boy whose father died when he was three. His mother works as a tea plucker. With a younger sibling to care for, the family struggled to meet even basic food needs.
IMHO began providing them with dry rations worth 3,000 rupees a month. The boy stayed in school.
When he sat for his Ordinary Level examinations, he scored nine distinctions!
When Dr. Rajam later visited the family, the boy’s mother made a simple request.
“She told me,” Dr. Rajam recalled, “‘Please share our story. I want people to know how much this “small” help has meant to us—how it has changed our lives!’”
Today, the boy is preparing for his Advanced Level examinations. He has long wanted to become a doctor. One can truly shoot for the stars when the environment is conducive to learning and growth.
His teachers say he is on track.
THE GEOGRAPHY OF CARE

IMHO’s work in Sri Lanka cuts across the ethnic geography that has long shaped humanitarian attention in the country.
The organisation has funded a psychiatric unit at Negombo Hospital, a Sinhala-majority town on the west coast. It has provided a dialysis machine to Ratnapura and supported cataract surgeries in Batticaloa, Kalmunai, Trincomalee, Nawalapitiya, Kegalle, and Dickoya.
“We do not look at race, religion, or ethnicity,” Dr. Thavam Thambi Pillai told me. “For us, everyone is human, and everyone has an equal right to live and receive care.”
“We stand true to our organisation’s name—the International Medical Health Organization,” he told me. “Suffering does not carry an ethnic identity—and neither should compassion. Health is a global language much like love and music.”
In practice, much of IMHO’s work remains concentrated in the Tamil-majority North, East, and upcountry regions, where decades of conflict and structural neglect have created the deepest gaps. But the organisation has never confined itself to those geographies.
“It goes where the need is real,” an IMHO official told me, “where there is a trusted partner on the ground—and where we can build something that will last beyond the intervention.”
HOW A CHARITY STAYS HONEST
One of the questions IMHO faces repeatedly is how an organisation that handles hundreds of thousands of dollars each year sustains the trust of the Tamil diaspora donors who fund it—despite the absence of institutional celebrity or government backing.
The answer, Dr. Rajam told me, is simple: paperwork and transparency.
IMHO is a registered 501(c)(3) nonprofit in the United States, subject to annual IRS reporting requirements. Its tax filings are public, allowing anyone to see how much the organisation receives—and how it is spent. At its twice-yearly public meetings—held in summer and autumn—the board presents a full accounting of expenditures, completed projects, and ongoing needs.
“I believe transparency and accountability are the main reasons people choose to support IMHO,” a long-time donor, who requested anonymity, told me.
That trust has proven resilient. During the Covid-19 pandemic—when charitable giving to many organisations declined sharply—IMHO’s donation levels remained largely stable.
Dr. Rajam attributes that consistency to years of credibility.
“When people see the impact,” she said, “they are moved to support.”
Not an End, but an Ongoing Work

It is March 2026. Nearly seventeen years have passed since the war that devastated Sri Lanka’s Tamil-majority North came to an end. Yet the work of reconstruction—physical, social, and psychological—remains unfinished.
Jaffna Teaching Hospital, with its 1,310 beds and more than 2,000 staff, now performs kidney transplants and bypass surgeries—procedures once unimaginable in the region —made possible in part through sustained support from IMHO. Beyond Jaffna, facilities such as the stroke unit in Chankanai , Arayampathy and the thalassemia unit in Batticaloa, Diabetic center in Kalmunai—and several others—continue to function with critical backing from the organisation.
At Jaffna Teaching Hospital, IMHO has introduced what is believed to be Sri Lanka’s first “befriender” programme. Trained young women are stationed at key entry points to guide patients—many of whom travel long distances from surrounding districts—through the complexity of a large tertiary-care facility. The idea came from local doctors. IMHO funded it.
In February 2026, Phase One of a new day surgery centre at the hospital was formally opened. The facility is expected to ease congestion and reduce the need for prolonged admissions, allowing patients to undergo procedures and return home the same day. As with many of IMHO’s initiatives, the concept originated with the university and hospital’s surgical team; IMHO secured the funding.
Elsewhere, at Maathavam—a centre for children with neurodevelopmental disorders that IMHO has supported since 2014—the organisation continues to strengthen services through training and long-term support.
And in Mullaitivu, the Iyankankulam primary healthcare centre—the first project IMHO ever built, in 2006—remains operational. Nearly two decades on, the organisation continues to step in when support is needed.
For IMHO, Dr. Rajam told me, this is what sustainability means: not a completed project, but a continuing relationship.
The Quiet Power of Small Acts
There is a story Dr. Rajam tells about a girl named Yalini from Sampur — a resettled area on the eastern coast where families had returned after nearly twenty years in displacement camps. They had been given thirty-five thousand rupees and some aluminium sheets by the government. They had no toilet and no access to clean water.
Yalini was a teenager with significant intellectual disabilities. Her older brother was physically disabled and visually impaired. Their mother's greatest fear, in the absence of a toilet, was that Yalini would have to go into the forest alone — and what might happen to her there.
When IMHO built toilets in the area, one went to Yalini's family. A common well was installed nearby. When Dr. Rajam visited again, Yalini showed her the toilet with such pride that the memory has stayed with her for years.
"Even a small intervention can restore dignity and safety — and truly change a life."
Nirosha is a Sinhalese woman who runs a small poultry farm with around four hundred chickens in Maskeliya. During the COVID-19 pandemic, she was unable to sell her eggs or afford feed. The farm was days away from collapse.
She came to IMHO—which does not normally support individuals—and they gave her a small amount to buy feed for a few weeks. All her chickens survived.
Today, Nirosha supplies up to two hundred eggs a day to an IMHO-supported cooperative store in Maskeliya, at below-market rates so the store can remain viable. She also volunteers at the vocational training centre, teaching sewing and bag-making.
Dr. Rajam tells this story when asked about goodwill and motivation. It is, in miniature, the logic behind IMHO’s work: that help does not end where it is given. It spreads. It returns. It takes new forms in other hands.
“That is the power of humanity!”
Dr. Rajam speaks easily about her father. He had grown up in poverty, never completing his education beyond the ordinary level, but he read voraciously and spent much of his life writing letters for those who could not—petitions to authorities, appeals against injustice.
She remembers him at his desk, sometimes skipping meals until a letter was finished. Though he grew up in poverty, he carried within him a deep sense of justice and compassion. He cared deeply about the suffering of others.
He taught her, she says, that indifference to suffering is not neutrality. It is a choice.
“I am a very ordinary person,” she says.
It is a line others repeat. Dr. Thavam Thampi Pillai says much the same. There is nothing extraordinary, they insist—only a belief that anyone can help, if given the opportunity.
“That,” an IMHO official told me, “is the organisation’s working philosophy.”
Somewhere in Maskeliya, a boy with nine distinctions at his Ordinary Level examinations is studying for his Advanced Levels. He wants to be a doctor.
Somewhere in Sampur, a girl named Yalini lives in a house with a toilet.
Somewhere in Jaffna, a man who had a heart attack last week—and who, in 2005, might have died because the road south was closed—is recovering in a hospital that now has the equipment and the doctors to save him.
These are not grand narratives.
They are the quiet, specific outcomes of twenty-three years of patient, unglamorous, volunteer-driven work—by people who asked themselves a question once, and never stopped answering it.