By: Dr Shane Halpe
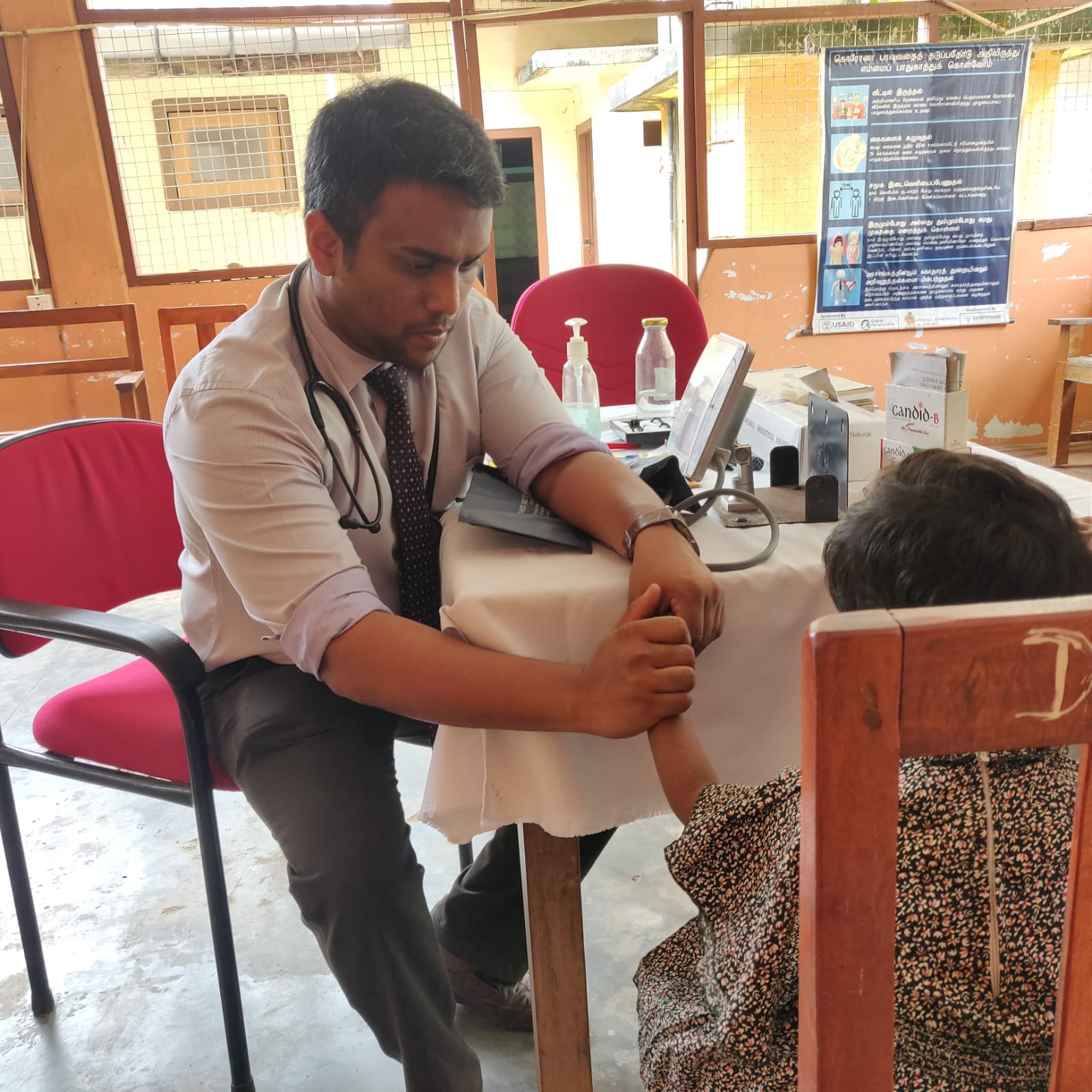
Batticaloa Teaching Hospital sits in the middle of a busy town—surrounded by roads, markets, schools, and the restless rhythm of everyday life. It is a place where ambulances arrive with breathless urgency, where families sit on benches holding reports and hope, where staff move quickly because delay has consequences. And yet, as Dr Mythily Barthelot—Deputy Director of the hospital—says with striking simplicity, the biggest challenge is not always the most dramatic one.
It is space.
Not the abstract kind of space we speak about in strategy meetings, but real, physical space—the absence of which can make even a well-staffed service feel like it is operating with one hand tied behind its back. “We have almost all subspecialties,” she explains, “but we are running short of space even though we have the consultants and the units.” Neurosurgical teams walk across wards to review patients. Some services exist, but without dedicated areas, they are forced into logistical compromises. And building upward is not always an option.
A hospital that learned to triage the future

Before speaking of expansion, Dr Barthelot speaks of systems—because systems, in her view, are what protect both patients and staff from chaos. The hospital’s A&E is one such system. Triage happens first. Patients are stabilised. Those needing closer monitoring go to the PCU. Surgical cases move through a short-stay unit and casualty theatres before reaching the wards.
It is an approach that sounds technical, but the principle is deeply humane: don’t push sick people into a maze. Organise care so that fear can be replaced with order.
Batticaloa Teaching Hospital, she reminds us, is not only serving the Eastern Province. Patients cross district borders—Ampara and beyond—because public hospitals in Sri Lanka do not ask for permission slips before offering care. The hospital’s oncology service is a major draw, particularly because it has a LINAC radiotherapy facility, a rarity that pulls patients from faraway districts. “There is no boundary,” she says, “people end up here.”
And yet, something quietly hopeful is happening too. OPD numbers are not exploding the way they do in some major hospitals, because peripheral primary care institutions within a 15-kilometre radius are functioning well. In other words, when the periphery strengthens, the centre can finally do what it is meant to do—handle emergencies, complications, and highly specialised care.
This is systems leadership in everyday language: strengthen what is near the people, so the tertiary hospital can focus on what only it can do.
From 1993 to 2025: a transformation that raises expectations
Dr Barthelot’s memory stretches back to the hospital’s earlier days. In 1993, there were only a handful of consultants. Now, she speaks of more than 56 consultants and over 250 doctors, and a hospital that has grown in subspecialties and capability.
Progress, however, has its price: expectations rise faster than infrastructure.
Even with expanded services, the hospital operates with a much smaller workforce than comparable teaching hospitals—about 1,800 to 1,900 total staff. They deliver “almost the same service” with “minimum human resources.” It is both a point of pride and a quiet warning: resilience can become a habit, but habit should not be mistaken for sustainability.
The boldest idea is not a building—it is a vision
When the conversation turns to development, Dr Barthelot refuses to think small. She does not speak about a new wing or a single ward. She speaks about land—fifteen acres, thirty acres—within a short drive. She speaks about relocating services that require space: rehabilitation, psychiatry, palliative care, waste management, and staff quarters. She even imagines a helipad, emergency transfer efficiency, and a regional centre that can attract trainees and electives from across Sri Lanka and beyond.
But the most striking part of her vision is not the architecture.
It is people.
Behind the hospital, families occupy land that the hospital could use for expansion. The easy solution would be eviction. Dr Barthelot proposes something profoundly different: a “Healthy Village” or “Hospital Village”—a planned resettlement with dignity, with double land, housing support, livelihoods, and integration into the hospital’s ecosystem. A win–win model where development does not require cruelty, and progress does not demand that the vulnerable be sacrificed.
Determination forged in the hardest classrooms
Her personal story explains why she speaks this way.
Dr Barthelot’s clarity comes from experience. She studied medicine in Russia. She returned to Sri Lanka determined to serve, only to encounter the harsh reality faced by many foreign graduates at the time: uncertainty, exclusion, and silence.
It was during this vulnerable period—when she aspired to sit the ERPM (then ACT 16) licensing examination—that mentorship became decisive.
At that time, Prof. Kandasamy Arulanandem was serving as Medical Officer (Grade I) – Public Health and Acting Deputy Director of Teaching Hospital Batticaloa. For foreign graduates, there was no structured pathway, no formal orientation, and little hope of clinical exposure.
“It was Arulanandem Sir,” Dr. Barthelot recalls with deep gratitude, “who helped me when we were completely helpless.” He opened doors that were otherwise closed, offering her the opportunity to gain orientation and training during her pre-intern period—an experience that proved critical for facing the licensing examination and for becoming the doctor and administrator she is today.
“I am ever grateful for his guidance and mentorship,” she says. In a system where rules often overshadow humanity, this act of mentorship changed a life—and, in many ways, continues to shape an institution.
Learning care from the margins
Her internship began in the North in 2009, just as the war had ended. The hospitals were overwhelmed. Resources were scarce. Typhoid outbreaks in IDP camps meant acute abdomen presentations surged. She describes being a single intern covering wards while theatres ran continuously. In Pallai, the hospital had been destroyed; services ran from a small house. Electricity was unreliable. Roads were damaged. Landmines made travel dangerous. A pregnant mother delivered in an ambulance that had no emergency kit.
She also speaks of learning community trust from an older RMO whom villagers called “Kadavul”—God. He did not begin consultations with laboratory values. He asked about mothers, sisters, cousins, even cows—because relationship came before prescription. At first, she felt irritated, sidelined, and ignored. Then she adapted. She wore sarees to look mature, asked about families, and met the community on their terms.
And suddenly, she was no longer an outsider.
The final lesson: service before self
Toward the end of my conversation with her, Dr. Barthelot’s message turns into a quiet challenge to the next generation. She expresses concern that some younger doctors may pursue rapid career advancement without cultivating the deep sense of service that once defined their mentors. Recalling the words of an elder, she says: “You are a public servant who delivers service. You are not merely doing a job.”
Her guidance is both simple and demanding:
Give your first two to three years fully to the nation.
Treat every patient as you would your closest friend.
Heal with respect and trust—not with medication alone.
Ask yourself each day: Am I ready to treat my own mother?
And perhaps her most radical counsel in an age obsessed with measurable outcomes: do not chase recognition. Do the work. Do it honestly. Let the outcome follow.